

What Does Prader-Willi Syndrome Mean? Understanding Symptoms, Causes, Diagnosis & Treatment
Medically reviewed by Dr. Natalie Hernandez, Pediatric Endocrinologist
Prader-Willi syndrome (PWS) is a rare genetic disorder that affects approximately 1 in every 10,000 to 30,000 births, making it one of the most common known genetic causes of life-threatening childhood obesity. Although many people associate Prader-Willi syndrome with an insatiable appetite and obesity, those features typically develop years after birth. The earliest signs are often much different, including severe low muscle tone, poor feeding, and delayed development.
Because Prader-Willi syndrome affects the hypothalamus, the area of the brain responsible for regulating hunger, hormones, growth, sleep, body temperature, and puberty, it can influence nearly every stage of a child's development. Early recognition and treatment can dramatically improve health, growth, mobility, and quality of life.
In this guide, we'll explain what Prader-Willi syndrome is, its symptoms, genetic causes, how it is diagnosed, and the treatments available today.
Quick Answer
Prader-Willi syndrome (PWS) is a rare genetic disorder caused by the loss of expression of specific genes on chromosome 15 inherited from the father. Children with PWS typically experience severe low muscle tone and poor feeding during infancy, followed later by excessive hunger (hyperphagia), obesity, short stature, hormonal deficiencies, developmental delays, and behavioral challenges. While there is currently no cure, early diagnosis, growth hormone therapy, nutritional management, and multidisciplinary care can significantly improve long-term outcomes.
What Is Prader-Willi Syndrome?
Prader-Willi syndrome is a genetic imprinting disorder. Unlike many inherited conditions, PWS is usually not passed from parent to child. Instead, it occurs because certain genes that should be active on the paternally inherited copy of chromosome 15 are missing or switched off.
These genes play a critical role in the development and function of the hypothalamus. When they are absent, the brain struggles to regulate several essential functions, including:
- Hunger and fullness
- Growth hormone production
- Puberty and reproductive hormones
- Sleep regulation
- Body temperature
- Muscle tone
- Energy expenditure
- Behavior and emotional regulation
This explains why children with Prader-Willi syndrome develop such a broad range of medical, endocrine, developmental, and behavioral challenges.
What Are the Symptoms of Prader-Willi Syndrome?
One of the defining characteristics of Prader-Willi syndrome is that its symptoms change with age. Many parents are surprised to learn that newborns with PWS often struggle to eat, while older children develop an overwhelming drive to eat.
Symptoms During Infancy
The earliest symptoms usually appear shortly after birth and may include:
- Severe low muscle tone (hypotonia)
- Poor sucking and feeding difficulties
- Weak cry
- Decreased spontaneous movement
- Poor weight gain or failure to thrive
- Genital underdevelopment
- Delayed developmental milestones
Some infants require temporary feeding tubes because they are unable to consume enough calories during the newborn period.
For pediatricians and neonatologists, unexplained hypotonia combined with poor feeding is one of the strongest reasons to pursue genetic testing for Prader-Willi syndrome.
Symptoms During Childhood
As children grow, the clinical picture changes dramatically.
Parents may begin noticing:
- Constant hunger
- Lack of normal feelings of fullness
- Rapid weight gain
- Short stature
- Small hands and feet
- Delayed speech and motor development
- Learning difficulties
- Mild to moderate intellectual disability
Without careful supervision of food intake, obesity can develop quickly because children with PWS have both an increased appetite and lower calorie requirements than their peers.
Symptoms During Adolescence and Adulthood
As children become older, additional endocrine and behavioral concerns often emerge.
These may include:
- Delayed or incomplete puberty
- Infertility
- Growth hormone deficiency
- Hypogonadism
- Obstructive sleep apnea
- Scoliosis
- Osteoporosis
- Type 2 diabetes
- Anxiety
- Obsessive-compulsive behaviors
- Skin picking
- Temper outbursts
- Rigidity with routines
Not every child develops every symptom, but the overall progression is remarkably characteristic of the condition.
What Causes Prader-Willi Syndrome?
Prader-Willi syndrome develops when genes that should be active on the father's copy of chromosome 15 are not expressed.
There are four primary genetic mechanisms responsible for this loss of gene function.
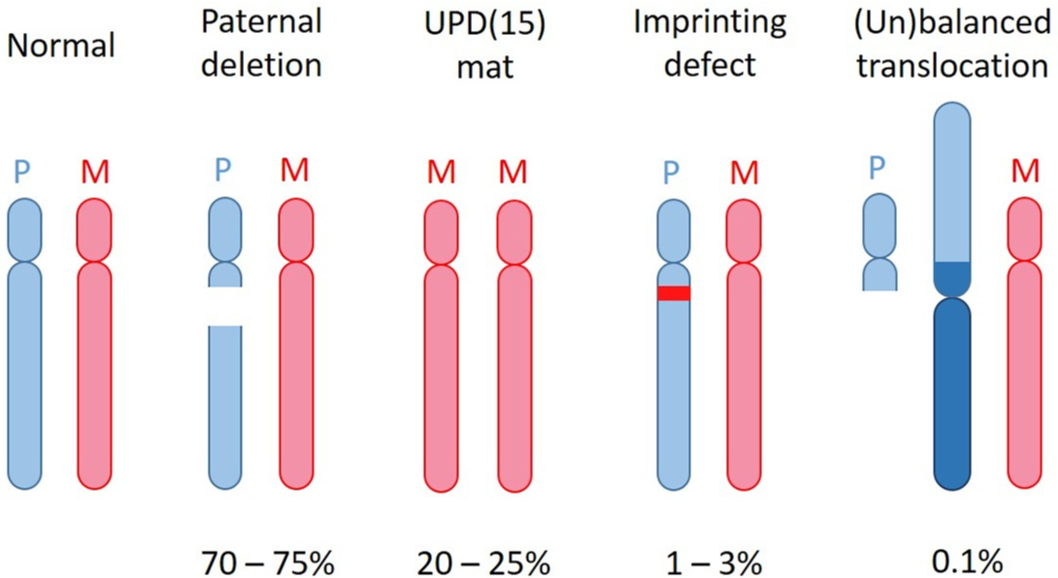
Figure 1. Ideograms illustrating the major genetic mechanisms responsible for Prader-Willi syndrome. Blue represents the paternal chromosome 15 and pink represents the maternal chromosome 15. The figure demonstrates paternal deletion, maternal uniparental disomy (UPD), imprinting defects, and rare chromosomal translocations. Adapted from Geets E, Meuwissen MEC, Van Hul W. Clinical, molecular genetics and therapeutic aspects of syndromic obesity. Clinical Genetics. 2019. Used under license from Wiley.
1. Paternal Deletion (65–75%)
This is the most common cause of Prader-Willi syndrome.
A small section of the father's chromosome 15 is missing, meaning several important genes are completely absent.
2. Maternal Uniparental Disomy (20–30%)
Instead of receiving one chromosome 15 from each parent, the child inherits both copies from the mother.
Because the paternal genes are missing, the affected genes are never expressed.
Children with maternal UPD often have slightly different behavioral characteristics than those with paternal deletions and may have a higher risk of psychiatric illness later in life.
3. Imprinting Center Defects (1–3%)
In these children, the paternal chromosome is physically present but is incorrectly "switched off."
This abnormal methylation pattern prevents important genes from functioning normally.
4. Chromosomal Translocations (Rare)
A very small percentage of patients develop Prader-Willi syndrome because chromosome 15 becomes rearranged with another chromosome.
Although uncommon, identifying these structural abnormalities is important because they may have implications for future family planning.
Why Does Prader-Willi Syndrome Cause Obesity?
One of the hallmarks of Prader-Willi syndrome is hyperphagia, an overwhelming, lifelong drive to eat.
Unlike typical hunger, hyperphagia occurs because the hypothalamus cannot properly recognize fullness after eating. Children may continue searching for food even after consuming a full meal because their brain never receives the normal "I'm full" signal.
Several factors contribute to weight gain in Prader-Willi syndrome:
- Constant hunger and reduced satiety
- Lower resting metabolic rate
- Reduced muscle mass
- Growth hormone deficiency
- Lower physical activity due to hypotonia
- Hormonal dysfunction affecting energy balance
This combination makes obesity one of the greatest long-term health risks for individuals with Prader-Willi syndrome. Fortunately, early nutritional guidance, environmental controls, growth hormone therapy, and ongoing endocrine care can significantly improve outcomes.
How Is Prader-Willi Syndrome Diagnosed?
Although a child's symptoms and physical examination may strongly suggest Prader-Willi syndrome, the diagnosis can only be confirmed through genetic testing.
Today, the recommended first-line test is DNA methylation analysis, which identifies more than 99% of Prader-Willi syndrome cases, regardless of the underlying genetic cause. Unlike older testing methods that looked for only one genetic subtype, methylation testing detects the abnormal gene expression pattern shared by nearly all individuals with PWS.
Once the diagnosis is confirmed, additional testing may be recommended to determine which genetic subtype caused the condition. This may include:
- Chromosomal microarray
- Fluorescence in situ hybridization (FISH)
- Multiplex ligation-dependent probe amplification (MLPA)
- Microsatellite analysis (often requiring parental DNA samples)
- Karyotyping if a chromosomal translocation is suspected
Determining the genetic subtype can help guide genetic counseling and provide insight into recurrence risk for future pregnancies.
How Is Prader-Willi Syndrome Treated?
Although there is currently no cure for Prader-Willi syndrome, advances in pediatric endocrinology have dramatically improved outcomes. The goal of treatment is to support healthy growth, optimize hormone function, prevent obesity-related complications, and help children reach their fullest potential.
Because PWS affects multiple organ systems, treatment is best coordinated through a multidisciplinary team that may include a pediatric endocrinologist, nutritionist, geneticist, developmental specialists, psychologists, physical therapists, and sleep medicine providers.
Growth Hormone Therapy
Growth hormone (GH) therapy is considered one of the most important treatments for children with Prader-Willi syndrome.
Rather than simply helping children become taller, growth hormone provides numerous health benefits, including:
- Improved linear growth
- Increased lean muscle mass
- Reduced body fat
- Improved muscle strength and mobility
- Better physical function
- Improved bone health
Current expert recommendations encourage starting growth hormone during infancy or shortly after diagnosis, provided there are no contraindications.
Because children with PWS have an increased risk of sleep-disordered breathing, a sleep study is typically recommended before starting growth hormone and repeated several weeks after treatment begins.
Nutrition and Weight Management
Managing nutrition is one of the greatest lifelong challenges for families affected by Prader-Willi syndrome.
Unlike most children, those with PWS often require significantly fewer calories while simultaneously experiencing a constant drive to eat. Successful weight management usually depends on both nutritional planning and environmental structure.
Families are often encouraged to:
- Establish consistent meal schedules
- Provide nutrient-dense, portion-controlled meals
- Limit access to excess food
- Encourage regular physical activity
- Create predictable routines around eating
Because hyperphagia is driven by changes in the hypothalamus—not simply a lack of willpower—families should never blame themselves or their child for these behaviors.
Hormone Replacement
Many children and adolescents with Prader-Willi syndrome develop additional hormone deficiencies that require treatment.
Depending on the child's evaluation, treatment may include:
- Sex hormone replacement during puberty
- Thyroid hormone replacement
- Evaluation for adrenal insufficiency when clinically indicated
- Ongoing endocrine monitoring throughout childhood and adulthood
Regular follow-up with a pediatric endocrinologist helps ensure these conditions are recognized and treated appropriately.
Developmental and Behavioral Support
Early intervention plays an essential role in helping children with PWS reach developmental milestones.
Supportive therapies may include:
- Physical therapy
- Occupational therapy
- Speech therapy
- Developmental services
- Individualized educational planning
- Behavioral therapy
- Mental health support when needed
Behavioral challenges, including anxiety, rigidity, obsessive-compulsive tendencies, and skin picking, often require individualized treatment plans that evolve over time.
Ongoing Monitoring
Because Prader-Willi syndrome affects many aspects of health, regular surveillance is important.
Children should be monitored for:
- Growth and body composition
- Thyroid function
- Blood sugar and diabetes risk
- Sleep apnea
- Scoliosis
- Bone health
- Pubertal development
- Vision problems
- Behavioral and mental health concerns
Routine monitoring allows problems to be identified early, often before significant complications develop.
Is Bariatric Surgery Recommended?
Despite severe obesity being a hallmark of Prader-Willi syndrome, bariatric surgery is generally not recommended.
Unlike obesity caused primarily by excess calorie intake, PWS results from impaired hypothalamic regulation of hunger and satiety. Surgical procedures do not correct this underlying brain dysfunction and may carry higher complication rates in individuals with the condition.
Instead, treatment focuses on comprehensive medical management, nutritional support, behavioral strategies, hormone replacement, and lifelong endocrine care.
What Is the Outlook for Children With Prader-Willi Syndrome?
There is no cure for Prader-Willi syndrome, but early diagnosis has significantly improved long-term outcomes.
Children who receive comprehensive care, including growth hormone therapy, nutritional guidance, developmental therapies, and endocrine management, often experience meaningful improvements in growth, body composition, mobility, and overall quality of life.
Although lifelong medical care is usually required, advances in genetics, endocrinology, and emerging therapies continue to improve the outlook for individuals living with PWS.
Frequently Asked Questions (FAQ)
Is Prader-Willi syndrome inherited?
Most cases occur spontaneously and are not inherited. However, rare imprinting center defects or chromosomal rearrangements may increase recurrence risk, making genetic counseling important for some families.
What is the first sign of Prader-Willi syndrome?
The earliest and most consistent sign is severe hypotonia (low muscle tone) with poor feeding during infancy.
Why are children with Prader-Willi syndrome always hungry?
The hypothalamus is unable to properly recognize fullness, resulting in hyperphagia, or an intense, persistent drive to eat.
Can Prader-Willi syndrome be cured?
No. There is currently no cure, but early diagnosis and multidisciplinary treatment can significantly improve health and quality of life.
Is growth hormone therapy recommended?
Yes. Current expert guidelines recommend growth hormone therapy for most children with Prader-Willi syndrome after an appropriate evaluation, as it provides benefits far beyond increasing height.
Key Takeaways
- Prader-Willi syndrome is one of the most common known genetic causes of life-threatening obesity.
- The earliest signs are usually low muscle tone and poor feeding, not excessive hunger.
- Hyperphagia typically develops later in childhood due to hypothalamic dysfunction.
- DNA methylation testing confirms more than 99% of cases.
- Growth hormone therapy is a cornerstone of treatment and improves far more than height.
- Lifelong multidisciplinary care can dramatically improve health and quality of life.
Concerned About Your Child's Growth or Development?
If your child has low muscle tone, feeding difficulties, excessive hunger, delayed growth, delayed puberty, or another endocrine concern, an evaluation by a pediatric endocrinologist can help identify the underlying cause and guide the next steps.
At LIFE Pediatric Endocrinology, our physicians specialize in caring for children with rare endocrine and genetic conditions, including Prader-Willi syndrome, growth disorders, thyroid disease, delayed and early puberty, obesity, and metabolic disorders. We believe that early diagnosis, individualized treatment, and proactive care can make a meaningful difference in a child's long-term health and quality of life.
Learn more or schedule a consultation
About Dr. Natalie Hernandez
Dr. Natalie Hernandez is a pediatric endocrinologist and Director of Metabolic Health and Obesity Medicine at LIFE Pediatric Endocrinology. She specializes in pediatric obesity, insulin resistance, type 2 diabetes, Prader-Willi syndrome, monogenic obesity, hypothalamic obesity, and other complex endocrine and genetic disorders affecting children and adolescents.
Dr. Hernandez is passionate about combining evidence-based medicine with compassionate, individualized care to help children achieve healthier futures. Learn more about Dr. Natalie Hernandez through her physician profile to explore her clinical expertise, research interests, and approach to pediatric metabolic health.
References
- Höybye C, Tauber M. Approach to the Patient With Prader-Willi Syndrome. Journal of Clinical Endocrinology & Metabolism. 2022.
- Shelkowitz E, Gantz MG, Ridenour TA, et al. Neuropsychiatric Features of Prader-Willi Syndrome. American Journal of Medical Genetics Part A. 2022.
- Butler MG, Hossain WA, Tessman R, Krishnamurthy PC. Preliminary Observations of Mitochondrial Dysfunction in Prader-Willi Syndrome. American Journal of Medical Genetics Part A. 2018.
- Cassidy SB, Schwartz S, Miller JL, Driscoll DJ. Prader-Willi Syndrome. Genetics in Medicine. 2012.
- Geets E, Meuwissen MEC, Van Hul W. Clinical, Molecular Genetics and Therapeutic Aspects of Syndromic Obesity. Clinical Genetics. 2019.
- MedlinePlus. Prader-Willi Syndrome. National Library of Medicine. 2022.
- Tauber M, Höybye C. Endocrine Disorders in Prader-Willi Syndrome: A Model to Understand and Treat Hypothalamic Dysfunction. The Lancet Diabetes & Endocrinology. 2021.
- Lionti T, Reid SM, White SM, Rowell MM. A Population-Based Profile of 160 Australians With Prader-Willi Syndrome. American Journal of Medical Genetics Part A. 2015.
- Gunay-Aygun M, Schwartz S, Heeger S, O'Riordan MA, Cassidy SB. The Changing Purpose of Prader-Willi Syndrome Clinical Diagnostic Criteria and Proposed Revised Criteria. Pediatrics. 2001.
- Driscoll DJ, Miller JL, Cassidy SB. Prader-Willi Syndrome. GeneReviews®. Updated 2024.
Share this

What Is Hypothalamic Obesity? Causes, Symptoms & Treatment

Prader-Willi Syndrome Facial Features: Signs & Symptoms
