

What Does a Child With Prader-Willi Syndrome Look Like? A Guide to Facial Features by Age
Medically reviewed by Dr. Natalie Hernandez, Pediatric Endocrinologist
If you're searching for "Prader-Willi syndrome face," you're probably wondering whether your child's facial appearance could be a sign of this rare genetic condition.
Children with Prader-Willi syndrome (PWS) often share several recognizable facial features, but no single facial characteristic can diagnose the condition. In fact, many children with Prader-Willi syndrome have subtle facial findings—or none at all. The earliest clues are often low muscle tone, poor feeding during infancy, and developmental delays, not facial appearance.
Understanding what to look for can help families recognize when further evaluation and genetic testing may be appropriate.
Quick Answer
Children with Prader-Willi syndrome may have a narrow forehead, almond-shaped eyes, a narrow nasal bridge, a thin upper lip, downturned corners of the mouth, and a long, narrow face. While these facial features are commonly associated with the condition, they are not present in every child and cannot confirm the diagnosis. Genetic testing remains the gold standard for diagnosing Prader-Willi syndrome.
Can You Recognize Prader-Willi Syndrome by Facial Features?
Prader-Willi syndrome has several characteristic facial features that experienced pediatric endocrinologists and geneticists may recognize during an evaluation. These findings are considered part of the classic phenotype but vary significantly from one child to another.
Common facial features include:
- Narrow forehead (narrow bifrontal diameter)
- Almond-shaped eyes
- Narrow nasal bridge
- Thin upper lip
- Downturned corners of the mouth, creating a triangular-shaped mouth
- Long, narrow face
Although these findings can provide helpful clues, studies have shown that the classic facial appearance is present in only about half of individuals with genetically confirmed Prader-Willi syndrome. This means many children with PWS may have only subtle facial differences or none at all.
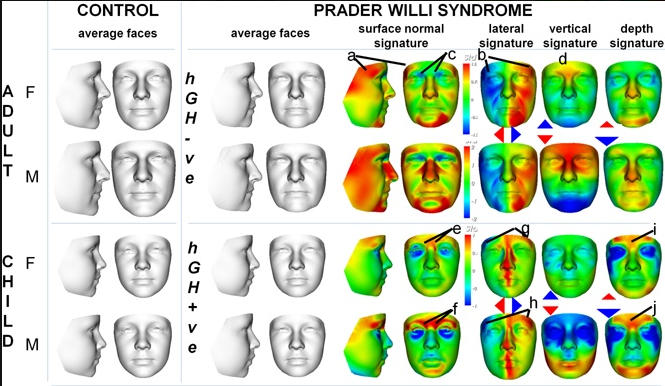
Figure 1. Three-dimensional facial analysis comparing children and adults with Prader-Willi syndrome (PWS) to age- and sex-matched controls. The heat maps demonstrate characteristic facial differences, including bitemporal narrowing, orbital positioning changes, and reduced overall facial dimensions. Adapted from de Souza MA et al. Growth hormone, gender and face shape in Prader–Willi syndrome. American Journal of Medical Genetics Part A. 2013. Used under license from Wiley.
Why Do Facial Features Change With Age?
One reason parents often struggle to recognize Prader-Willi syndrome is that facial features evolve over time.
During infancy, the face may appear relatively typical. As children grow, differences in facial bone development and soft tissue become more noticeable, allowing the classic appearance to gradually emerge.
Researchers have also found that growth hormone therapy may influence facial development, meaning children treated early often have less pronounced facial differences than untreated adults. This is one reason facial appearance varies considerably between individuals.
Facial Features by Age
Infants
Facial features are often subtle during the newborn period. Instead, physicians are much more likely to notice:
- Severe hypotonia (low muscle tone)
- Poor sucking and feeding
- Weak cry
- Excessive sleepiness
- Poor weight gain
These findings are much more important than facial appearance when deciding whether a newborn should undergo genetic testing.
Toddlers and Young Children
As children grow, facial characteristics often become easier to recognize.
Parents may notice:
- Almond-shaped eyes
- Narrow forehead
- Thin upper lip
- Downturned corners of the mouth
- Long, narrow face
Developmental delays and speech delays also become more apparent during this stage.
Adolescents
The characteristic facial appearance often persists into adolescence, although body composition changes and obesity may alter the overall appearance of the face.
By this age, behavioral symptoms, hormonal abnormalities, and hyperphagia usually become much more significant than facial features alone.
Not Every Child Looks the Same
Prader-Willi syndrome can occur through several different genetic mechanisms, and these differences may influence facial appearance.
Children with the classic 15q11-q13 deletion often have more recognizable facial features than those with maternal uniparental disomy (UPD). They may also have lighter hair and fairer skin than other family members because of the loss of genes involved in pigmentation.
Even among children with the same genetic subtype, however, facial appearance can vary considerably.
Other Physical Features Beyond the Face
While many parents first notice facial differences, pediatric endocrinologists evaluate the whole child rather than focusing on appearance alone.
Other common findings include:
- Small hands and feet
- Short stature (if untreated)
- Low muscle tone
- Delayed or incomplete puberty
- Developmental delay
- Scoliosis
- Strabismus (crossed eyes)
- Genital hypoplasia
Taken together, these findings provide much stronger evidence than facial features alone.
The Earliest Signs Parents Should Watch For
One of the biggest misconceptions about Prader-Willi syndrome is that it is first recognized by facial appearance.
In reality, the earliest and most important signs usually occur before the facial features become obvious.
Birth to 2 Years
Parents and healthcare providers should watch for:
- Severe hypotonia
- Poor feeding
- Weak suck
- Poor weight gain
- Delayed motor milestones
Ages 2 to 6 Years
As children grow, families often notice:
- Increasing appetite
- Developmental delays
- Speech delays
- Facial features becoming more recognizable
School Age and Beyond
Older children may develop:
- Hyperphagia (an intense drive to eat)
- Rapid weight gain and obesity if food access is not controlled
- Learning difficulties
- Anxiety
- Obsessive-compulsive behaviors
- Skin picking
- Temper outbursts
- Sleep disturbances
This progression is so characteristic that experienced specialists often recognize the syndrome based on the overall clinical pattern rather than facial appearance alone.
Can You Diagnose Prader-Willi Syndrome by Looking at a Child's Face?
No.
Although facial features can raise suspicion for Prader-Willi syndrome, they should never be used to confirm or exclude the diagnosis.
Current expert recommendations encourage a low threshold for genetic testing, particularly in newborns and infants with unexplained hypotonia and poor feeding.
The most accurate test is DNA methylation testing, which identifies more than 99% of Prader-Willi syndrome cases.
If your child has developmental concerns in addition to some of the facial or physical features described above, discussing genetic testing with your pediatrician or pediatric endocrinologist is appropriate.
When Should Parents Seek an Evaluation?
You should speak with your child's healthcare provider if your child has:
- Severe low muscle tone
- Difficulty feeding as a newborn
- Developmental delays
- Small hands or feet
- Excessive hunger beginning in early childhood
- Poor growth
- Facial features concerning for Prader-Willi syndrome
Early diagnosis allows children to receive nutritional support, developmental therapies, hormone evaluation, and growth hormone treatment when appropriate. Earlier intervention has been shown to improve health, physical development, and long-term outcomes.
Frequently Asked Questions (FAQ)
Are almond-shaped eyes enough to diagnose Prader-Willi syndrome?
No. Almond-shaped eyes are one of several facial characteristics associated with Prader-Willi syndrome, but they are also seen in many healthy children. They should never be used as the sole basis for diagnosis.
Do all children with Prader-Willi syndrome have the same facial appearance?
No. Facial features vary by age, genetics, growth hormone treatment, and individual development. Some children have very subtle findings.
Does growth hormone therapy change facial features?
Research suggests that early growth hormone treatment may reduce the severity of some facial differences while improving growth, muscle mass, body composition, strength, and overall health.
Is genetic testing necessary?
Yes. Because facial features alone are not reliable, DNA methylation testing remains the gold standard for diagnosing Prader-Willi syndrome.
The Bottom Line
Searching for "Prader-Willi syndrome face" is often the first step many parents take when they notice differences in their child's appearance. While children with Prader-Willi syndrome frequently have a recognizable pattern of facial features—including almond-shaped eyes, a narrow forehead, a thin upper lip, and a long, narrow face—these findings alone are not enough to make the diagnosis.
The earliest and most important clues are usually low muscle tone, poor feeding during infancy, developmental delays, and later the onset of excessive hunger. When these signs occur together, prompt evaluation and genetic testing are essential.
At LIFE Pediatric Endocrinology, we believe early recognition leads to earlier treatment and better outcomes. If you have concerns about your child's growth, development, or hormonal health, our team is here to help.
About Dr. Natalie Hernandez
Dr. Natalie Hernandez is a board-certified pediatric endocrinologist and the Director of Metabolic Health and Obesity Medicine at LIFE Pediatric Endocrinology. She specializes in pediatric obesity, insulin resistance, prediabetes, type 2 diabetes, Prader-Willi syndrome, monogenic obesity, and other genetic and metabolic disorders affecting children and adolescents.
Dr. Hernandez believes in treating the whole child, not just the diagnosis, using evidence-based medicine and compassionate, individualized care to help children achieve lifelong health.
Learn more about Dr. Natalie Hernandez →
Concerned About Your Child's Growth or Development?
If your child has unexplained low muscle tone, developmental delays, excessive hunger, or features concerning for Prader-Willi syndrome, an early evaluation can make a meaningful difference.
At LIFE Pediatric Endocrinology, our pediatric endocrinologists provide comprehensive evaluations for children with rare endocrine and genetic conditions, including Prader-Willi syndrome, growth disorders, obesity, delayed puberty, thyroid disease, and more.
Schedule a consultation today to learn how our team can help your child receive an accurate diagnosis and personalized treatment plan.
References
- MedlinePlus. Prader-Willi Syndrome. National Library of Medicine. 2022.
- Tauber M, Höybye C. Endocrine Disorders in Prader-Willi Syndrome: A Model to Understand and Treat Hypothalamic Dysfunction. The Lancet Diabetes & Endocrinology. 2021.
- Oldzej J, Manazir J, Gold JA, et al. Molecular Subtype and Growth Hormone Effects on Dysmorphology in Prader-Willi Syndrome. American Journal of Medical Genetics Part A. 2020.
- Martínez JB, Arancedo JMÁ, Solari A, et al. Classic Prader-Willi Syndrome Phenotype Caused by an Atypical Deletion in the 15q11 Region Not Involving the SNORD Genes. Clinical Genetics. 2025.
- Gunay-Aygun M, Schwartz S, Heeger S, O'Riordan MA, Cassidy SB. The Changing Purpose of Prader-Willi Syndrome Clinical Diagnostic Criteria and Proposed Revised Criteria. Pediatrics. 2001.
- de Souza MA, McAllister C, Suttie M, et al. Growth Hormone, Gender and Face Shape in Prader-Willi Syndrome. American Journal of Medical Genetics Part A. 2013.
- Mahmoud R, Leonenko A, Butler MG, et al. Influence of Molecular Classes and Growth Hormone Treatment on Growth and Dysmorphology in Prader-Willi Syndrome. Clinical Genetics. 2021.
- Driscoll DJ, Miller JL, Cassidy SB. Prader-Willi Syndrome. GeneReviews®. Updated 2024.
- Höybye C, Tauber M. Approach to the Patient With Prader-Willi Syndrome. Journal of Clinical Endocrinology & Metabolism. 2022.
- Moy VF, Denton JJ, Bohonowych JE, Strong TV. The Motivations and Methods Behind Sharing a Pediatric Prader-Willi Syndrome Diagnosis. American Journal of Medical Genetics Part A. 2024.
Share this

What Is PMOS (Formerly PCOS)? Symptoms, Diagnosis & Treatment in Teens

5 Hormone-Disrupting Ingredients Endocrinologists Recommend Avoiding
